


If this leaked document is authentic, RFL-100, Aviptadil, seems to work. Of course, a simple plasma transfer can easily kill Covid19, and a vaccine or two that have been around since a few weeks after the virus was discovered work as well (and everyone is waiting for Vaccine government approval, and NOT as we are told waiting for a Vaccine (as if it was being worked on in a lab every day)).
But in case a patient is left to deteriorate to the point damage to the lungs is the issue, it seems Relief Therapeutics, which in part works to limit inflammation and the cytokine storm, and perhaps even to limit viral replication in the lung cells, may be a very effective treatment.
Previous data was already quite promising, but this document makes it a home run. The question is, is it authentic? If it is not, though I have not had a chance to analyze it carefully yet, it would be a very impressive forgery due to many factors clearly evident in the document.
A further question, from an economic perspective, is what would be the value. VIP is a naturally occurring peptide. That aside, this virus will soon not only be quite rare, but vaccines will be available as well. On the other hand, the hysteria would push it to shocking highs in the near term upon any positive news from the administration or FDA, and it has potential benefits to ARDS and related conditions in non covid-19 related cases.
What say you?
Update Aug 23 2020
The short answer is “Yes”, that document was relatively authentic. It appeared to be an earlier draft of their release that leaked prematurely.
The company, upon learning of it and preparing the final official draft, requested a halt in trading (on Aug 20, too late for having an significant effect), and released the official version with a warning that the earlier document was not official.
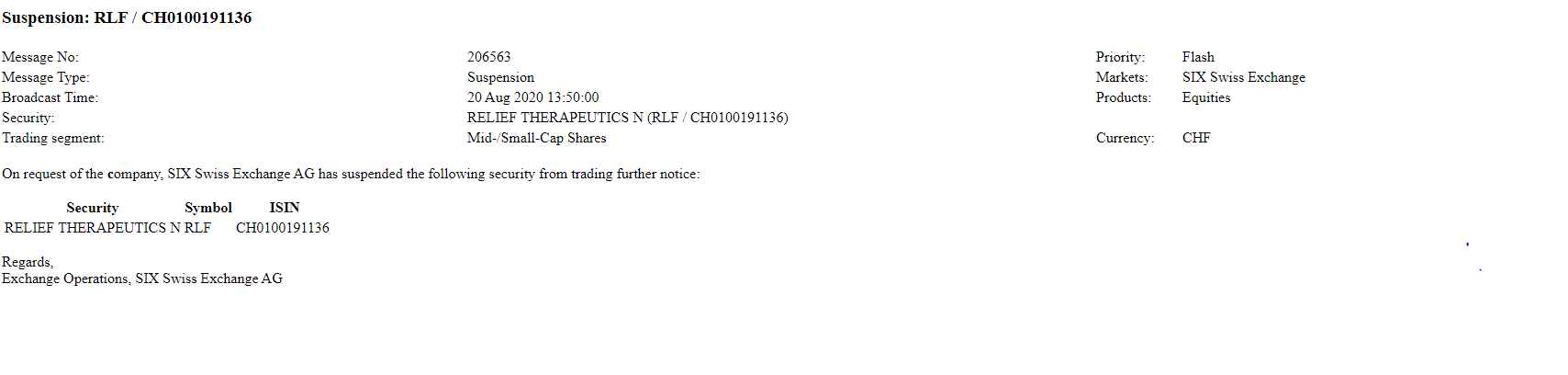
The official document is the following:
The differences are not major, there are some details that vary, as does some of the tone and stile (not surprisingly after a more formal review), but the bottom line data is quite similar in both documents.
The biggest difference is the official version adding the following section at the end of the document:
These results should be interpreted in light of the understanding that only a minority of those infected with SARSCoV-2 develop COVID-19. The finding that survival in those with COVID-19 respiratory failure is correlated with natural levels of VIP is particularly thought-provoking.1 If SARS-CoV-2 can be prevented from infecting and replicating in vulnerable nasopharyngeal and pulmonary cells that display ACE2 surface receptors, coronavirus is potentially a low-threat pathogen to humans, as it is to other mammalian species. Indeed, while non-human mammals can be infected with SARS-CoV-2, none seem to develop lethal COVID-19.
Our findings suggest that patients with earlier stage disease and an intact pulmonary epithelium may benefit from inhaled aviptadil in order to prevent progression to respiratory failure. FDA has granted an inhaled use IND and a phase 2/3 trial of inhaled aviptadil (NCT04360096) is about to commence. Aviptadil may have further value as a nasopharyngeal drug to prevent SARS-CoV-2 from successfully infecting nasopharyngeal cells and starting the pathogenic process of COVID-19. Moreover, aviptadil may have promise in treating a broad array of pulmonary inflammatory conditions.
Unlike expensive-to-produce monoclonal antibodies and difficult-to-scale convalescent plasma, VIP can ultimately be produced at a cost of pennies per dose, if moved from peptide synthesis to yeast fermentation, as is done for insulin. As such, it may represent a critical therapeutic for COVID-19 and possibly other viral infections for both the developed and the developing world.
Below is a comparison of both files for those who are interested in noting all the differences in detail:
Possible Trump Announcement
There is a much anticipated Presidential announcement scheduled for later today. President Trump has hinted at this announcement for some time and mentioned it may have to do with therapeutics.
The likely candidates for this announcement are:
- CytoDyn Inc’s (CYDY) Leronlimab as a CCR5 antagonist
- Swiss Relief Therapeutics’ (RLF) RLF-100 or Aviptadil
- Convalescent Plasma
The first by Cytodyn is (hopefully), the least likely candidate in the announcement because it has the weakest data. The management of the company is unusual to put it mildly, and their data release very incomplete. Though the UK has recently accepted the drug for a phase 3 trial, all that really means in these hectic times, is that they considered it safe enough to test the efficacy. As has been covered extensively in my blog in the past, and from the very begging many months ago (and as the last section of RLF’s paper quoted above reminded us as well), our present coronavirus is a weak virus in general terms and an anti-viral effect in general is not what is needed for the proportionally small segment of the population that is suffering from its potential effects on the lungs. Lung tissue damage, inflammation and certain immunological responses such as cytokines, are what require targeting in such a case. These hard-to-get-to areas of the lung are being damaged, and can lead to death by the mere lack of oxygen.
CytoDyn’s product does not have the robust data thus far, and seems to be on a less likely mechanism of action track to success in the needed cases.
Like I predicted at the very outset of the epidemic, drugs and treatments will be very difficult to test when done so in small scale and in any manner other than large, double-blind and controlled studies (which is very difficult in the life-or-death situations available given the horrendous government controls), because most people get over the virus. An immense majority get over the virus without issue at all, many without even knowing they were infected, and those that suffer from mild and severe cases also largely overcome the disease. Only in a minority of severe cases, even counting only those cases where patients are receiving mechanical ventilation and/or oxygenation, are the results ultimately fatal. Because of that, depending on the population being tested, along with a myriad of factors surrounding them (age, general health and comorbidity factors for example), as well as the regular quality of care, many drugs can “appear” to work or reduce the chances of fatality.
There is a reason debates rage on about many of these therapeutics including… it’s not easy to tell if a drug works or not when a disease rarely kills you.
Leronlimab I suspect, largely fits into this model…as likely does the much more famous Remdesivir. They may help marginally in certain cases (and if applied at certain times), but when the body can easily overcome this mild or weak virus in the general system, in the vast majority of the population, the drug needed by the majority in mortal danger must specifically target the condition of the lungs and either the viral activity or immunological activity therein (if not both).
Convalescent Plasma may very well be the subject of the Trump announcement if only because it would be in the style of the president to “hit back” after the recent (and shocking) FDA announcement to stop (or “place a hold”) on its Emergency Use Authorization of the treatment. I have discussed plasma much more thoroughly in previous blogs, and hope to shortly do an even deeper dive into the issue shortly, so will not expand much further here. Suffice to say, that convalescent plasma, at least if given to matching patients and donors (matching in various parameters up to including the strain of the virus in the matching process) and using plasma of a sufficiently strong antibody mix and concentration works.. and works almost a priori.
It may fail to reverse the damage of people whose lung function is already massively decimated, and certainly will not typically reverse the various conditions severe patients may find themselves in (a patient may still be 86 years old, and still be suffering from cancer, hypertension and diabetes even after receiving antibodies geared to fight the covid-19 viurs!) but it certainly will stop the virus in its tracks, within the patients general system. If given early enough, to a patient who really is in mortal danger from the coronavirus, and not from various other ailments, it ought to save them almost without question.
Finally, this is where RLF’s Aviptadil comes in. The reports they have released go beyond the typical placebo effects we have seen elsewhere. The mechanism of action of this naturally occurring peptide is logical, and supported by the various blood markers tested in the blood and reported in their findings. It intends to work exactly where patients in severe cases require it, in the lungs.. where it seems to act as anti-viral, anti-inflammatory and tissue protection/healing agent. These may be related or sperate functions in the mechanism but the early data support.
Outside of plasma, I have not seen any therapeutic with this kind of clear data supporting its efficacy. Convalescent plasma, and vaccines may have been around for a while, basically from the start of the epidemic (and still waiting for governments’ approval), but as far as an actual therapeutic, RLF’s product is the closest I have seen thus far. The closest frankly, had simply been steroids (which are like magic and work in a myriad of situations where “manning up!” is what the body requires), which also significantly improve odds of someone in a severe case pulling through.
Due to all of this it would be interesting to see if indeed RLF is what President Trump mentions, perhaps as part of a product purchase deal, though I still think plasma may be his man announcement do to the recent activity around it and President Trump’s nature. Perhaps he will announce more than a single candidate.
If RLF’s Aviptadil and Plasma are the kind of therapeutic he will mention, he will be in the right side of science… hopefully he will stay away from mentioning more far fetched products that may amount to little more than quackery.
Update:
So it was convalescent plasma.
RFL’s Aviptadil may still be mentioned in the future, especially if they continue to report periodically before their early October clinical trial. Of course, the virus will be withering away fast, and with upcoming vaccine approvals coming as well, the value remaining to RLF (and others working on therapeutics) will be in question. In this case, it does have some potential value for other ARDs situations outside of covid-19 cases.
As for the plasma, as I have written before, it is shocking that it was restricted at all more than half a year after the start of the pandemic, and kudos for Mr. Trump for quickly bashing the FDA into submission on this issue. At least partially. It was clear from the press conference that this is what happened and Mr. Trump used and diverted some of the vultures in the room, to attack the FDA.
Of course, Mr. Trump can “collude” with his FDA employees to direct their actions and decisions, and in this case he has done so in the right direction. Plasma data is still limited due to the very restrictions imposed by the government. If at the very least, they had used their restrictive state powers, to have allowed all use for willing patients, but required thorough recording of data, there would be hundreds if not hundreds of thousands times more data than needed on this (and other) treatments.
For example, it stands to reason that if older people and people at higher risk received plasma as soon as they were infected (a sort of pseudo-vaccine), they would not deteriorate to a severe case where the lungs are damaged and mortality is a high risk (and to a point where neither plasma nor other treatments could help). It also stands to reason that giving the right mix of antibodies and concentrations is also important. The media makes a big deal of “neutralizing antibodies” but that is by no means the story. Firstly, we do not know all antibodies that are neutralizing nor to what extend they are neutralizing. Secondly, antibodies do not have to themselves be neutralizing to work, in fact the classic mode of action of antibodies is simply to “flag” foreign bodies in the system for other agents of the immune system to take care of. It turns out that “killing” or even completely digesting a virus or bacteria, no matter how dangerous, is the easy work… (we have enzymes to break down steak, we can easily break down any virus), the hard part is knowing what to destroy and what NOT to destroy. Auto-immune diseases are an example of this going awry. It is the same for drugs as the immune system. You can destroy HIV, covid and flesh eating bacteria on a counter-top at a whim (with anything from alcohol and bleach to a blowtorch), but it’s harder to find something that will do the same without killing a patient as well.
In any event, if doctors would have recorded the various relevant characteristics of patients, their condition before receiving plasma, as well as the nature of the plasma being used (antibodies present, concentration… and ideally PCR data from the virus originally present in the donor), the data would easily have shown proven and highly effective plasma-related treatments many times over by now… and in fact would have done so by the second and most likely the first month of the pandemic.
The current restrictions of the various emergency use authorizations, are not only absurdly (and immorally) restrictive, and require a large amount of red tape to get through, but also fail to require a good standard of data to come out of the emergency use. Typical case of government at work, it is no surprise of course, but it is surprising that we hand over our liberties to its like even when it comes to life and death situations of ourselves and our loved ones.
One more item of note in the press conference was Dr. Hahn’s obtuse explanation of the 35% fatality reduction. In either ineplty trying to explain how significant that is or in pretending to want to do that, he stated that if 100 people are sick, and 35 survive that would be pretty significant.
That is insane for lack of a better word, and incorrect. In the case of this virus for example, if you have 100 people who get infected, let us say 95 will survive (just making up a number here as an example, it would of course depend on the medical characteristics of these 100 and that number could be much better or a bit worse depending on who those folks are), and 5 will die. The 35% fatality reduction would mean that 35% of those 5, having given plasma, would now survive. The new total being about 97 people surviving and 3 dying (instead of 5).
His remarks would indicate clearly to the uninformed that out of 100 people infected with this hyped up virus, 35 could potentially survive thanks to this new Trump authorization, and only 65 perish…! Whereas previously, I guess all 100 would have died. This clown heads the FDA and on a daily basis holds the lives and fortunes of millions in his hands.
Take a look for yourself (as of posting, starts at about 1 hour and 17 minutes):
Facebook Comments
WordPress Comments
Disqus Comments